Peripheral nerves have the ability to regenerate. The injured nerve fiber (axon) is very long and it has to regenerate and reach its target in a reasonable time so that the patient can have a good function (Figure 1). The nerve has protective layers of tissue surrounding it.

The epineurium surrounds the nerve itself. The perineurium is located around the fascicle (Figure 2). The endoneurium is located around the axon.

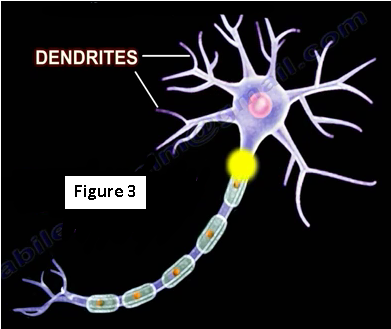
A motor neuron fiber’s axon transmits signals to a muscle or a gland. The neurons become stimulated at the dendrites (Figure 3). Neurons possess structures that allow for the transmission of impulses and are composed of two parts; the receiving structures and the conducting structures. The receiving structures are the cell body and the dendrites. The conducting structures are the axon terminal and axon.
Signals from the brain are passed on to the muscles in the limbs by these motor neurons (Figure 4).

When a painful stimulus is applied to a sensory receptor in the skin (afferent), the information is transmitted to the central nervous system (CNS). Once the sensory signal has been received by the CNS, another signal is then sent from the brain (efferent) and passed along the motor neurons in order to move the muscles in response to the painful stimuli (Figure 5).

When the nerve is affected or cut, there will be no function of that nerve (Figure 6). When the axon is separated from the body, there will be degeneration of the axon and the degeneration will stop at the synapse and will not travel to the next neuron. Regeneration of the peripheral nerve is possible and all events of regeneration occur around the axon when the nerve is cut. The proximal stump will regenerate and the distal stump will have Wallerian degeneration. Macrophagocytes dispose of the degenerated axon and myelin sheath.

Peripheral nerves have Schwann cells and endoneurium that helps in regeneration. Schwann cells grow into the cut area and join the two ends.
The entire axonal material is phagocytized from the site of the injury to the endplate. A new generated axon sprouts and grows to reestablish the connection for reaching its target (Figure 7).

Wallerian Degeneration
The neuron is able to survive and regenerate after the axon has been cut with neuronal survival and Wallerian degeneration. The Wallerian degeneration typically arises from severe nerve injury such as axonotmesis or neurotmesis. The cell body increases in size with migration of the nucleus towards the cell periphery. The cell body enlarges for approximately 20 days and remains enlarged until axon regeneration is complete. In the proximal part of the nerve segment, degeneration can occur and it is proportionate to the severity of the injury. Degeneration extends proximally to the next node of ranvier. Wallerian degeneration is seen in the distal portion of the nerve fiber (Figure 8).

Axonal degeneration is followed by degradation of the myelin sheath and infiltration by macrophages. The macrophages are accompanied by Schwann cells which clear the debris from degeneration. Distally, you will find Schwann cells proliferate and the axon sprouts (finger-like growths) and advance (Figure 9). Using Schwann cells as a guide, these sprouts advance about 1 mm per day. Atrophy of the associated muscle can be seen during the process.

Axonal growth is seen and the connection is reestablished with the muscle appearing to be bigger and a bit healthier. When the axon fails to establish continuity, a neuroma formation will be seen with no regeneration of the axon distally. Atrophy of the associated muscles will be seen during the process (Figure 10).

There are three types of nerve injuries: Type I (neurapraxia), Type II (axonotmesis), and Type III (neurotmesis).
Neurapraxia
The prognosis is good with neurapraxia and it is the mildest form of nerve injury and the nerve remains intact (Figure 11).

Axonotmesis
This type of injury is severe. The axon is damaged and the surrounding connective tissue remains intact (Figure 12). There will be partial or complete recovery of the nerve and Wallerian degeneration occurs distal to the injury site. Recovery occurs 1 mm per day or 1 inch per month.

Neurotmesis
There will be no recovery with neurotmesis. Fibrillation is present and the injury usually requires surgery (Figure 13). Motor neuron until potential is usually absent. In neurotmesis there will be degradation and neuroma formation.

There are several factors that affect the success of recovery. If the gap between the proximal and distal stumps is too wide or scar tissue has formed, surgery can help to guide the sprouts to the tube. Some of the factors that are favorable for nerve recovery after repair include younger age of the patient, distal injury, no significant delay in repair, sharp cuts (better than a crush), vascularity is preserved (Figure 14), and favorable orientation of the nerve in epineural repair.

For more information on nerves, follow the links below:
Radial Nerve Injury, Locations
Nerve Injury, Injuries Complete
Nerve Injury, Positions of the Hand
For more information, visit my YouTube Channel:
Originally published at www.huffingtonpost.com on February 24, 2017.