
This piece was first posted on Substack. To comment, please go there.
Suburbs can be terrific places. I live in a suburb, and I can think of few better places to live, to raise a happy, healthy family. Suburbs represent stability, and the ascent of the middle class, a trend which significantly broadens access to the material resources that support health. Indeed, when we speak about creating a world that generates health by expanding access to these resources, the ideal would be for everyone to be able to enjoy the level of wellbeing reflected by suburban life.
However, this is not yet the case—far from it. This unfairness is enforced by policies that benefit those with more at the expense of those with less. It is also enforced by habits of thought that allow us, even if we consider ourselves progressive-minded, to oppose measures which would share some of our advantage with others. Sadly, perhaps inevitably, there is a racial element to this, just as there is to the broader gap between the rich and the poor, and addressing this challenge means speaking honestly about the full dynamics of the issue, including its intersection with race. I was struck by an article written last summer by former Minneapolis Mayor Betsy Hodges, where she tackled this uncomfortable truth, saying, “White liberals, despite believing we are saying and doing the right things, have resisted the systemic changes our cities have needed for decades. We have mostly settled for illusions of change, like testing pilot programs and funding volunteer opportunities.”
Such observations are, I think, bracing and necessary. It is easy to see how ideological opponents can block progressive change; it is perhaps more difficult to see how our own blind spots can help stymie progress. Today’s column, then, will address the suburban impulses that can sway those of us who are committed to the pursuit of justice off the path that leads to better health for all, and how we can resist these impulses, to create a healthier world.
What do I mean by suburban impulses? Fundamentally, they are captured by an acronym: NIMBY or “not in my backyard.” NIMBYism is when people living in a community oppose measures which would support the public good in that community when these measures would in some real or imagined way encroach on their own personal convenience (I have written previously about NIMBYism here). A corollary is that this opposition can come from people who would otherwise support such measures, as long as they happen somewhere else.
A classic example of NIMBYism is its emergence in the context of affordable housing. Safe, affordable housing is a necessary condition for health, core to a progressive vision for a healthier world. Yet when the prospect of building affordable housing arises in communities, including communities where the political composition is broadly left-leaning, pushback can emerge against building units within these places. This pushback can be informed by concern over property values, over changes to the physical layout of the community, or it can indeed be fueled by animus toward the prospect of people of a different race/socioeconomic position moving into town.
This hypocrisy plays into the depiction of suburbs we often see in books, films, and television shows as places of artifice, in which a sunny exterior hides less appealing truths. Many fictionalized depictions of this can be quite dark, although I have always preferred the more comedic framing of the film The Truman Show. The film depicts an idealized suburban life for its protagonist, Truman Burbank, who learns in the course of the story that his life is, in fact, an elaborately staged reality television program. While NIMBYism does not neatly match the premise of The Truman Show, both fact and fiction are linked by the phenomenon of communities appearing to be one way and then being revealed to be another.
Why does this matter to public health, and, in particular, to the vision of a liberal public health these columns aim to support? Fundamentally, it matters on two levels. First, any action in the social or policy space which is motivated by wariness towards “the other,” or even by racism and hate, is bad for health. When these attitudes animate our thinking about how we shape our communities, they undermine the capacity of these communities to be as healthy as they can be, and further jeopardize the health of the vulnerable, those who are already being excluded from the resources that generate health. Second, it entrenches the impulse that pulls us away from change, causing us to resist progress in favor of a status quo which does not equally distribute health. It is more than a failure of policy or compassion, it is a failure of imagination—the ability to imagine a community which puts the good of all ahead of the fears and prejudices of some. Changing communities, changing the world, for the better means first being able to imagine such change. We cannot do so with NIMBY blinders on.
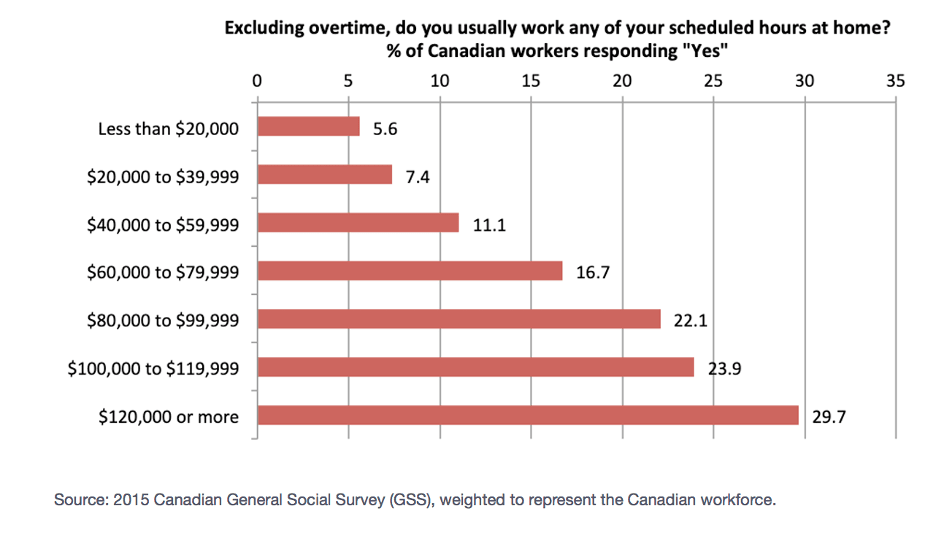
It is important to note, however, that our suburban impulses are not always characterized by the explicit rejection of measures that support the common good. Sometimes we are simply acting from a position of privilege to support measures we think are an unalloyed good for all, but that are actually onerous to those who live outside the picket fences of suburban comfort. We saw this during COVID-19, particularly in the conversation around lockdowns. Throughout the pandemic, those most able to navigate lockdowns were those living in safe, stable communities with plenty of space, material resources, access to electronic communications, and just enough distance from urban centers to justify an extended period of working from home: in short, those living in suburbs. And it was those who lacked these advantages for whom extended lockdowns were particularly trying. It was also the case that remote work was much easier for those working in the kind of high-wage professions which support a suburban lifestyle and harder for those working in the sales and service jobs that tend to pay less. The below data are taken from the 2015 Canadian General Social Survey. While the data predate the COVID moment by a number of years, they are nevertheless instructive in showing how higher income can translate into greater time working remotely, with those making $120,000 or more significantly likelier to spend time working from home than those making less than $20,000.
This divide reflects the extent to which socioeconomic privilege shapes the means by which we have been able to navigate the pandemic. Those able to work from home were clearly in one place on the socioeconomic ladder and those less able to do so were on another. Yet this divide was not what most of us talked about when we talked about whether or not to embrace restrictive lockdowns.
This begs the question: were those of us with a suburban mentality more willing to accept restrictive COVID rules because our relative comfort shielded us from their full consequences? It would be understandable for us to see the situation this way. From this privileged perspective, there is relatively less downside to ongoing lockdowns than there would be for someone who has fewer options for working from home. This is not to say, of course, that working from home is entirely without costs for those living in the suburbs, particularly for those with children. But the cost/benefit analysis is radically different when seen from both sides of suburban/non-suburban divide.
How can we resist our suburban impulses, to make sure we are supporting policies which work for the good of all, not just for the privileged? Core to doing so, it seems to me, is the old saying, “To whom much is given, much is expected.” We have a collective responsibility to ensure that the policies we pursue are policies which support the health of as many people as possible. What is perhaps ironic here is that many of those who have advocated for indefinite lockdowns likely felt that this is precisely what they were doing—advocating for the policy that was most conducive to the health of all. They were able to feel this way because their socioeconomic advantages made it difficult to see how it could be otherwise. This speaks to the importance of understanding the context that shapes health, so we can recognize when this context has positioned us to perhaps less-clearly see the extent of our privilege. We can then use our position to advocate for polices which truly support the health of all.
This reflects the motivation behind what has emerged as a counter to NIMBYism: the YIMBY (“yes, in my backyard”) movement. A YIMBY mentality argues for creating communities which are in the best interests of everyone, where the resources necessary for health, particularly housing, are widely accessible. Those of us who already enjoy access to these resources have a responsibility to not lose sight of when self-interest may be coloring our thoughts about the issues that matter for health. We can then recalibrate, to argue for a vision of health without divides—whether those divides are racial, economic, or a picket fence.